Are Prescription Drug Prices Becoming As Meaningless As Hospital Charges?
Professor Jack Hoadley of Georgetown University recently gave an excellent presentation discussing prices of prescription drugs. Two slides stand out. First, a slide showing how much prescription spending is controlled by insurers and governments versus patients directly:
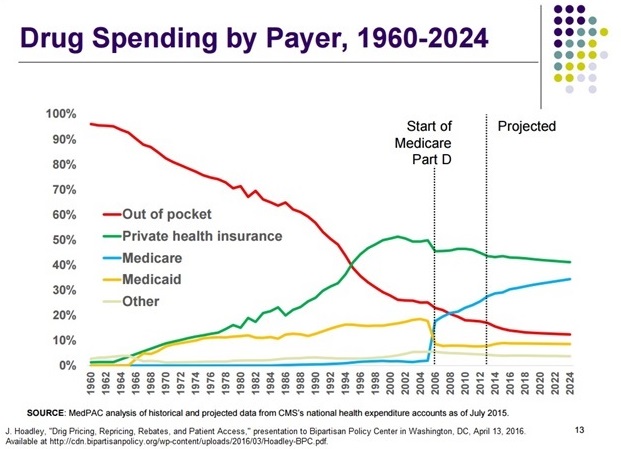
As recently as 1990, patients controlled over half of drug spending. Today, it is under 20 percent. Has this cost shift made drugs more “affordable”? Obviously not: 8 percent of patients do not take medicines as prescribed, because of cost. Hillary Clinton promises to impose government price controls on drugs if she becomes president.
The second slide shows rebates given by drug makers to insurers in Medicare Part D, the prescription benefit that was launched in 2006:
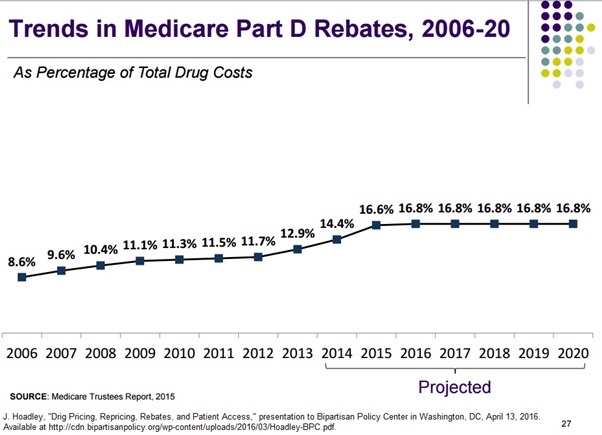
Rebates have almost doubled from 8.6 percent to 16.8 percent. In other words, if a drug maker says it charges $10 for a drug, it actually receives $8.32 from the insurer.
There is a lot of discussion these days about price transparency. However, it appears price transparency is very difficult once third-party payers (governments and insurers) dominate spending. After decades of being dominated by third-party payers, hospital charges are meaningless. On average, hospitals charge Medicare 3.77 times more than what Medicare pays, with a range of 0.42 times to 16.23 times. In other words, if a hospital sends a claim to Medicare for $10,000, the hospital is most likely to be paid $2,653, but they payment could be as little as $616 or as much as $23,810.
This has evolved over the years as a kind of symbiosis: It allows insurers to assert they are negotiating impressive discounts from hospitals; and allows hospitals to complain they are being pinned to the mat by insurers. Both actually do pretty well out of the arrangement.
A few years ago, patients benefitted from low, transparent prices for generic drugs dispensed by pharmacies. The $4 prescription is still a mainstay of retail pharmacy. Unfortunately, prescription pricing is becoming less transparent as government expands its reach.


Since I became eligible for Medicare at the start of 2012, I’ve been tracking the drug prices for all the drugs I take. I get a 90 day supply of my maintenance drugs by mail through UNH’s PBM, Optum Rx. After several years of relative price stability and even some price declines, prices for five out of six drugs rose dramatically at the start of this year even though all have numerous competitors. Here are the price changes from last October to the start of this year by drug: Bisoprolol, +100%; Amlodipine, +44.4%; Clopidogrel, +119.8%; Isosorbide Mononitrate, +84.7%; Simvastatin, +67.3%; and Enalapril, -5.5%. Prices are the sum of what the plan paid plus my coinsurance amount. It doesn’t make any sense to me. What gives? At the same time, my monthly premium for 2015 is up 77.8% from what it was in 2012. What a deal!!
When the drug companies succeeded in getting Medicare Part D, they thought they had solved the problem of seniors complaining about high prescription costs, because they would be largely socialized. Apparently, they were too optimistic, because drug prices are in the public eye more than ever.
UNH also noted that it currently administers approximately $80 billion in annual drug spending of which $30 billion or 37.5% is for specialty drugs. I think payers need to be prepared to exclude some of these drugs from their formulary if their in house medical experts tell them the net price after discounts and rebates exceeds the value in improved patient outcomes vs. alternative therapies.
Perhaps, but it is also the case that some (or many) of these specialty drugs have unique benefits. If some patients cannot get them, there may not be adequate substitutes.
Sounds like a death panel to me.
For the most part, generic drugs respond to the fundamentals of economics. There is a definite correlation between the number of generic competitors and the average price compared to the brand drug prior to patent expiration. Brand drugs not so much. Back when every drug maker sought to develop so-called “me-too” drugs for chronic diseases, brand drugs were also quite competitive relative to the brand drug when no competitor existed. Now that nearly nine-in-ten drugs taken are generic; and the FDA is encouraging drug makers to develop specialty drugs for rare conditions, the prices often seems about as meaningless and hospital prices. I think part of the reason is that 1) the market for innovative drugs is only 11% of the market; 2) biotech drugs enjoy stronger patent protections. Increasingly, drug makers have to create fewer high tech drug and price them like superstar blockbusters — whether they are or not.
Another fine example of what happens when the government intervenes to “help” us. It’s doing for prescription drugs what it did for healthcare. Hiding and skewing real costs. Please “help” me a lot less.