Why Are U.S. Prescription Prices Higher?
 Jeanne Whalen of the Wall Street Journal has written a feature article comparing U.S. prescription drug prices to those overseas. Unsurprisingly, she find prices in other developed countries lower, and credits government price controls in other countries with (pretty much) all the difference.
Jeanne Whalen of the Wall Street Journal has written a feature article comparing U.S. prescription drug prices to those overseas. Unsurprisingly, she find prices in other developed countries lower, and credits government price controls in other countries with (pretty much) all the difference.
A vial of the cancer drug Rituxan cost Norway’s taxpayer-funded health system $1,527 in the third quarter of 2015, while the U.S. Medicare program paid $3,678. An injection of the asthma drug Xolair cost Norway $463, which was 46% less than Medicare paid for it.
Drug prices in the U.S. are shrouded in mystery, obscured by confidential rebates, multiple middlemen and the strict guarding of trade secrets.
The state-run health systems in Norway and many other developed countries drive hard bargains with drug companies: setting price caps, demanding proof of new drugs’ value in comparison to existing ones and sometimes refusing to cover medicines they doubt are worth the cost.
(Jeanne Whalen, “Why the U.S. Pays More Than Other Countries for Drugs,” Wall Street Journal, December 1, 2015)
I do not dispute the facts of the article, but the article’s misidentifying the primary reason why drug prices are different. It actually does a good job of differentiating countries where the state exercises monopsony power over drug purchases (like Norway) and those where the state does not exercise purchasing power, but imposes price controls on al sales (like Canada). It is easy and intuitive to conclude that such government interventions reduce prices. However, contrary evidence shakes that thesis. Relative purchasing power better explains the difference.
I showed this by example in a paper I wrote 15 long years ago, in which I compared prices for other goods and services which are the fruit of intellectual property. The markets for these goods and services are substantively the same in Canada and the U.S. Despite this, Canadian prices were significantly discounted (Table 3).
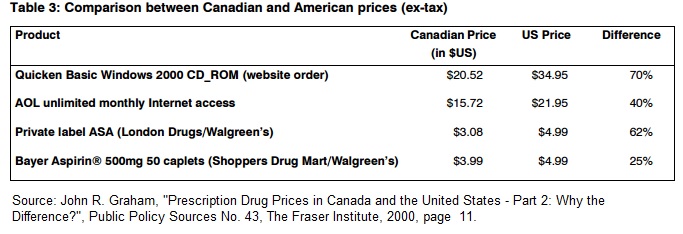 No law forced Intuit to sell the Canadian version of Quicken significantly cheaper than the U.S. version. It was just what the profit maximizing price was, given market conditions.
No law forced Intuit to sell the Canadian version of Quicken significantly cheaper than the U.S. version. It was just what the profit maximizing price was, given market conditions.
Let me throw in a couple of other observations. As noted in the article, the prices of goods which do not contain a lot of intellectual property (or, perhaps more property stated, for which manufacturing and distribution costs are a very high share of total cost per unit) are lower in the U.S. than other countries. I won’t try to go through the entire argument in this blog post, but it is clear that the prices of groceries, gasoline, clothing, et cetera, are not lower in the U.S. because the government drives a hard bargain on consumers’ behalf. No, they are low because of competitive markets.
Further, the prices of all these items, even a simple can of soda pop, “are shrouded in mystery, obscured by confidential rebates, multiple middlemen and the strict guarding of trade secrets,” as the article describes the prescription market. I am referring, of course, to items like Coke® or Pepsi®, which nobody argues are expensive. The difference in market structure between soft drinks and prescription drugs is that consumers spend their own money directly on the former, instead of through insurers and government. Nor does it take 12 to 15 years to get a new soft drink on the market to compete with incumbent suppliers, like it does for prescription drugs.


In a paper published by NCPA in 2005, Alain Enthoven argued that bargaining power was essentially the power (and willingness) to say “no” and deny a customer your business. Some of the countries with socialized medical systems have the ability to decide a given drug (although beneficial) does not save as many life years as another drug. For example, let’s consider a cancer drug extends life by two months and costs $100,000. That adds up to $600,000 per life year saved. But another drug extends life by 1 month, but costs $10,000, that’s only $120,000 per life year saved. To the government, $120,000 is a better deal. But to the patient, an extra month for $480,000 is a bargain.
Having seen a lot of cancer patients in the last month of life, I’m not sure I’d agree with that. When you keep flogging dying people, you’re usually not doing it for them but for the family members who won’t let go.
http://www.zocalopublicsquare.org/2011/11/30/how-doctors-die/ideas/nexus/
To me, the end of life care question becomes what, if anything, can doctors do to make family members more willing to let go? For example, would it be helpful if they provided an honest diagnosis without instilling false hope? Could they be quicker to say I’m sorry but there is nothing more that we can do? Could they find diplomatic ways to raise the cost issue? Could they better explain to the family member(s) that, at this point, we are doing more TO the patient than FOR the patient and he/she is suffering as a consequence? To complicate matters, doing more means that both doctors and hospitals get paid more. I’m sure the hospitals in particular like that as long as the care is kept within their system and not referred out to a competitor. The drug companies obviously like it too.
True dat. Some docs don’t know when they’ve transitioned from prolonging life to prolonging death, families can be very obstinate and threatening, and raising the cost issue can make you seem mercenary. You can’t really say, “Let’s turn off Granny’s ventilator because she’s costing us a fortune”.
OTOH, I’m having trouble with the fuss over the cost of new hepatitis C drugs like Harvoni. A course of interferon/ribavirin therapy is 48 weeks and the cure rate is less than 50%. The side effects of interferon can be terrible. It causes the most profound depression I’ve ever seen.
Harvoni is a 12 week course with a 90% success rate. Harvoni is a true game-changer that will decrease morbidity and mortality significantly.
The high price of Harvoni is much easier to justify than Lidoderm patches, which I consider band-aids with lidocaine in them that cost $150+ for 30 patches. Lidoderm is OTC in Canada and costs less than $10.
Micheal, I just switched an old 2003 MSA client today and on the app I put Hep – C treatment for 3 months in 2014 with 100% cured. My wife says the underwriter will want to postpone but I don’t know. If they are cured are they cured?
The guy said he was surprised that TIME Insurance approved the cost at just under $100,000 for the Rx.
There are several issues regarding the pricing of Sovaldi and Harvoni that I think warrant consideration and discussion. First, while Gilead Sciences may have made a reasonable argument regarding the pricing of these drugs vs. previously existing treatments for Hepatitis C, the potential patient base is very large vs. diseases that other expensive specialty drugs were developed to treat. Specifically, Hepatitis C afflicts three million people in the U.S. alone and 150 million worldwide. Of the U.S. patient base, 17% are in prison as I understand it. If the drug were made widely available to as many patients as possible, the adverse budget impact on payers, including Medicaid, would be huge.
Second, as a financial person, I often ask how profitable do drug companies need to be to attract capital and earn a sufficient risk-adjusted return on that capital to appropriately compensate investors for the risk they took in buying the company’s stock? Drug companies will tell you that their primary duty is to their shareholders which accounts for why they try so hard to maximize shareholder value. However, it should be noted that patients buy these drugs because they have to and not because they want to. For that reason, I think the drug companies should try to strike a better balance among all stakeholders and not just try to squeeze every last possible nickel out of the marketplace.
Finally, the willingness of drug companies to sell their drugs for significantly lower prices in other countries, including other developed countries, creates significant ill will among Americans. They will say they are pricing based on ability to pay and they use per capita GDP as a proxy for ability to pay. However, to my knowledge, no other industry prices its products that way. In my opinion, it’s obnoxious behavior at best.
The article has more than one specific example: Quicken financial planning software, which cost more in the U.S. than Canada. Not only do industries to this across borders. then do it in domestic markets.
Segmenting customers to differentiate pricing is Marketing 101.
“Segmenting customers”
That is something that seems to have always been around, but in healthcare many consider that type of practice distasteful to the point that they would invade personal freedom to get rid of it. Why?
My daughter with MS is currently having issues and is changing from the shots she gives herself to going into a center every three months and doing an intravenous procedure. Each time she goes it costs $20,000. She says the sky is not falling and her research indicates remarkable results. I hope so.
At 1:30 yesterday I talked with Stephanie Carlton who is Jeb’s Healthcare Policy Adviser. I asked her if there was somebody on the campaign that knew the law and was involved with the free market. Steph said, “I take offence to that question because I know all of the laws.” I said, “OK, Jeb was my Governor and Florida’s law is that an employer cannot pay one penny of the premium for an employee to get personable and portable Individual Medical (IM) but must purchase dangerous over-priced employer-based insurance that they lose if a hurricane blows the business away. It’s a State created crisis. There is no COBRA extension if the business is blown away, right?” Steph said, “I’m not going to answer that question.”
Then I asked Steph, “If the business owner has a heart attack and wants to sell his 7-Eleven, he loses his employer-based insurance so he can’t sell, right?” Steph said, “I take offence to that question.” I told her, “You can’t say that, that makes no sense.”
I told Steph about my daughter and how people need permanent insurance before I asked my questions. Steph said that I can’t know who else is on the healthcare policy team because it is private. So, no transparency in the Sunshine State when people run for President.
Like Jimmy Buffett says, “Give me something tall and strong make it a hurricane before I go insane. Its only half past 1 but I don’t care – it’s 5 o’clock somewhere.”
I don’t endorse politicians, but I am happy to endorse Stephanie Carlton – one of the best health staffers around.
Maybe you are one of the secret people on the debate prep team John.
It is Federal ACA Law that prohibits the employer from paying for an Individual Policy. Not Florida State Law. (although there could be some type of overlaying State Law…..) If the company is blown away in a hurricane and the group insurance policy ceases to exist, there would be no COBRA but all individuals would be eligible for the off Open Enrollment Special enrollment into any individual plan at that time. No preexisting conditions would apply and you would be able to research which carriers would cover the needed drug before enrolling.
In follow up, the same thing with your question of the guy that wants to sell his business. The minute he cancels or becomes ineligible for the 7-11 group insurance policy, he has a ticket to immediately enroll in an individual plan. No waiting periods or pre existing conditions.
Paula, you’re a hoot. Don’t you remember Small Group Reform creeping across the Nation lead by those traitors NFIB in the late 1990’s? It was State law in every State. You are wrong it is still Florida law because they have not changed it. You are talking about current law and SEP (Special Enrollment Period). I was talking about Jeb as Governor of Florida in the pea-picking-past before your SEP. Everybody and their dog knows that today a hurricane would produce an SEP so employees could purchase over-priced and heavily mandated Obamacare plans with sky-high deductibles that you so dearly love. You California girls…
“it is clear that the prices of groceries, gasoline, clothing, et cetera, are not lower in the U.S. because the government drives a hard bargain on consumers’ behalf. No, they are low because of competitive markets.”
Does it matter that you can import all those things from other countries? How much would clothing cost if you could only buy American-made clothes? How about cell phones, cars, steel, oil? You can’t buy medication from Canada.
Actually, a lot of the medication you buy legally comes from Canada. GSK, for example manufactures vaccines in Canada. Most global pharma companies have manufacturing in Canada and the Canadian factories have global mandates to supply one or more medicines. It is a global market.
What you are talking about is illegal piracy, like buying DVDs on the streets of Bangkok.
The prices in the US are high because the Pharma industry has manipulated Congress in the passing of the rules and laws. I believe each company has a right to sell their product or service in a free economy for whatever price they believe they can charge from a free and willing public. The key word here is a “free economy”. The drug business is not a “free economy, it has been manipulated to the benefit of the Pharma industry and they are capitalizing on their manipulation to the detriment of businesses and individuals and benefit of their shareholders.
Why do I say this? Simple:
– the ACA mandates medications be included in the health plan.
– The health plan must cover almost all medications that are FDA approved.
– Health plans can not exclude the new expensive medications that provide improved outcomes.
– Medications can only be purchased from US based suppliers, not the most inexpensive suppliers.
– While health plans use tools such as Prior Authorization, Step Therapy and other cost control mechanisms, over time the MD’s and patients very often still end up receiving the most expensive drugs.
– The maximum out of pocket in a health plan now includes Rx copays and expenses. The impact of charging higher copays or increased costs to the participant for the very expensive drugs is mitigated very early on. In essence, once a participant meets their out-of-pocket maximum all expenses are covered at 100%. Having them pay more for a more expensive option and then making the decision if it is worth the extra price or not is removed.
Putting this together, the ACA mandates that drugs have to be covered. There is no choice. The buyer (insurance companies) have to buy from a limited supplier and pay whatever cost is charged. Not exactly free trade or an arms length transaction.
So in summary, Pharma has a rigged game and they are taking advantage of it to the detriment of everyone other than their shareholders and there is not a damn thing we can do about it.
A couple more fun items:
– Pharma advertises heavily in direct to consumer advertising. Some estimations are advertising and marketing expenses are more than 3 times the amount spent by Pharma on R&D.
– the US is one of two countries in the developed world that allow direct to consumer drug advertising. Why? They create unnecessary demand from a consumer that a third party is mandated to pay for with little to no recourse.
I don’t believe government should mandate what a product should cost nor put price controls on it. What I do want is for the restriction of having to cover all medications, regardless of cost, removed and allow for medications to be purchased from any country/source that meets the FDA requirements. Let the drug companies charge what they want, just let me buy them from a source that has negotiated the best price possible and have the freedom to say, it isn’t worth the cost and we’re not going to include it as a covered medication.
Thank you. I accept a lot of your argument. The whole health system is a mess of government intervention and every participant is trying to maximize their income.
I disagree with your accusation against advertising. Most items that are heavily advertised to a mass public are inexpensive. Pizza delivery is heavily advertised in both local and national markets. Yet pizza delivery is inexpensive.
It is not the advertising, but government intervention that drives up the costs.
“It is not the advertising, but government intervention that drives up the costs”
And not only the US government.
Which reminds me of another factor that has not been mentioned: how pharmas allocate their drug development cost.
Allocating virtually all of that cost to US markets, where there are no price controls, allows pharmas to show a profit in other countries that have price controls, even when they sell the same drug at a much lower price than in the US. It also means Americans bear virtually all the cost of drug development. I believe this is true for US – based pharmas; I suspect it’s true for other pharmas, as well.
If US pharmas were to allocate a share of their drug development cost to other countries, they would not recover all of it if any of those other countries did not allow the drug on the market. Being shut out of another country’s market becomes more likely as the drug price rises, and drug prices would rise if they had to bear a share of the drug development cost.
Price regulation by other governments is one reason the pharmas jump thru these hoops.
It’s often said that price regulation in the US would chill new drug development here. It might also mean significant price increases in other countries – yet another perverse outcome of government regulation.
Actually, the worlds medical research budget is about 300 billion dollars. The US covers less than half that, not “virtually all”. US research is also about 45 % government-funded. Pharmas allocate less money to research in the US than they do to advertising.
Also, there are slightly more huge pharmas in Europe than in the US.
Further, US research seems to be much like the rest of the healthcare sector in that huge amounts of funding does not necessarily result in better results. The US seem to be better at commercializing or improving breakthroughs than making them.
The EU publishes more biomedical research than the US (Although US research is cited more -but citations heavily favour English-language papers)
Finally, when pharmas and European nations negotiate drug prices, that does not mean that pharmas sell at a loss, they simply sell at a lesser profit.
A drug company researches drugs that will sell. They won’t refuse to sell a drug to a customer base of 7 billion at a profit of 1 cent per pill because they aren’t allowed to sell to 320 million at a profit of 100 times that.
Drug research have nothing to do with US prices. The pharmas charge Americans more because Americans let them
No other area of high-cost research requires human sacrifice to function.
“It’s often said that price regulation in the US would chill new drug development here. It might also mean significant price increases in other countries – yet another perverse outcome of government “
I think that’s exactly right, John. I would be willing to bet a lot of money that if the U.S. had price regulation or, more likely, if private insurers and pharmacy benefit managers were more willing to refuse to cover expensive specialty drugs at current prices because they’re not willing to stick the U.S. population with the full cost of drug company R&D anymore, prices would go down in the U.S. and increase overseas.
The drug companies would just go to the appropriate authorities in Europe and elsewhere and explain that they can no longer load the full cost of R&D solely on U.S. customers so you folks are now going to have to cover your fair share of R&D costs. Hence, higher prices for other developed countries to offset lower prices in the U.S. I don’t know why this hasn’t already happened years ago.
Why do we need price fixing by government or all that intervention? Because government likes to control and that control is expensive. How long would Canada be able to demand a lower prices for pharmaceuticals if the American consumer or their agent were able to buy those pharmaceuticals in Canada as easily as Canadians?
Total nonsense. Plus you missed what is by far the biggest fact.
Our prescriptions cost so much more, mostly because FDA approval averages $350 million and takes 12 years on average. In fact, that high cost is why rarely used drugs are so costly here. Divide that $350 million among a mere 100-200 American patients.
No country comes close the our FDA approval, in both dollars and time. And, no, American pharmaceuticals would be crazy to recover their overhead in America, with higher prices everywhere elae.
My much simpler take is we (the US) subsidize the world’s pharmaceuticals. Or conversely the world sucks at the teat of America. In the case of the 3rd world nations (say, nearly every country in Africa), this is on balance a good thing. When you live on a buck a day, you can’t swing the price of AZT to stay alive. And out of compassion the US has provided it. But wouldn’t it be great if Norway, arguably the richest nation on earth, chipped in?
The entire worlds biomedical budget is ~300 billion dollars. The waste in the US healthcare system is about 1500 billion, five times as much.
So even if the US did all the research on the planet, it’d still be way too little to explain US healthcare costs.
In practice, the US covers less than half the spending, although on a per person basis, Americans do contribute the greatest amounts to research.
However, the US healthcare system is well known for costing more without performing better, and there are indications that this is also the case for the research part of it.
More research happens in Europe (although once again, the US does more per person), most big breakthroughs come from elsewhere, and the number of Nobels per person is low. US research in general seem better at commercializing or incrementally improving breakthroughs from elsewhere.
In the area of US research finance, the biggest single contributor is actually the government, and the pharmas spend more on advertising than research.
I think you underestimate the importance of price elasticity. (The ability of the customer to refuse a product if the price is too high). If the can of soda is too expensive, you don’t buy a can of soda. If your 5-year old needs a million dollars worth of cancer treatments, you will do anything -anything- to raise a million dollars.
Note that competition works quite well to reduce prices in areas such as vanity surgery and lasik. And even in high-cost countries such as Norway (with the 10-dollar beers) private healthcare is much cheaper than in the US, as the customer can simply chose to use public facilities if the cost becomes unreasonable.