National Health Spending Slowdown Underwhelms; Obamacare Hurting Middle Class
Last week, the media got more than usually excited about the latest National Health Expenditures (NHE) produced by actuaries at the Centers for Medicare and Medicaid Services (CMS). Modern Healthcare reported that “healthcare spending growth hit 53-year low in 2013,” noting that last year’s 3.6 percent growth was the lowest since 1960.
While it is literally true that last year’s increase was the lowest since 1960, growth in 2009 was only 3.8 percent, after 4.8 percent in 2008. You do not need a PhD in economics to conclude that the recession was likely the largest factor. It is hard to detect much more than noise in the annual changes since the recession hit. This is corroborated by the fact that 17.4 percent of Gross Domestic Product is accounted by health care ― exactly the same percentage as in 2009 and every year since.
Nevertheless, CMS’ actuaries allege that Obamacare’s provisions kept a lid on costs, citing:
- productivity adjustments for Medicare fee-for-service payments;
- reduced Medicare Advantage base payment rates;
- increased Medicaid prescription drug rebates; and
- the medical loss ratio requirement for private insurers.
Yes, Medicare spending dropped from 4.0 percent in 2012 to 3.4 percent in 2013. However, Medicare’s enrollment growth also slowed, and the Republican-driven sequestration also held back spending. Medicare spending per enrollee actually rose at the same rate as in 2012. It is hard to see Obamacare’s technocratic cost savings in these figures.
Medicaid spending exploded 6.1 percent. Although government wrangled more discounts from drug makers, this did not compensate for increased Medicaid enrollment and higher fees for providers. The best performance was by private insurers, for whom spending growth dropped from 4.0 percent in 2012 to 2.8 percent in 2013. Medicare regulates health insurers’ medical loss ratio (MLR), which is the ratio of medical claims to total premium (actually, a more complex calculation than it appears). CMS’ actuaries credit this regulation with lowering the growth of private insurers’ spending.
As Greg Scandlen explains, the MLR regulation is actually a disguised way to cause consumers to make interest-free loans to health insurers. Robert Book of the American Action Forum has discussed how the MLR regulation could actually increase insurers’ profits. It is all to do with accounting entries, not reducing the actual costs of care. If the rate of spending growth by private insurers is slowing, it is surely caused by something else.
That something is likely consumer-driven health care. NCPA’s Health Policy Blog has discussed much evidence of consumer-driven plans keeping cost growth down. The latest report, from Mercer, reports that consumer-driven plans covered 23 percent of beneficiaries in the employer-based market in 2013. This is up from 3 percent in 2006 and 11 percent in 2010. Employers and employees are attracted to these plans because they manage costs better.
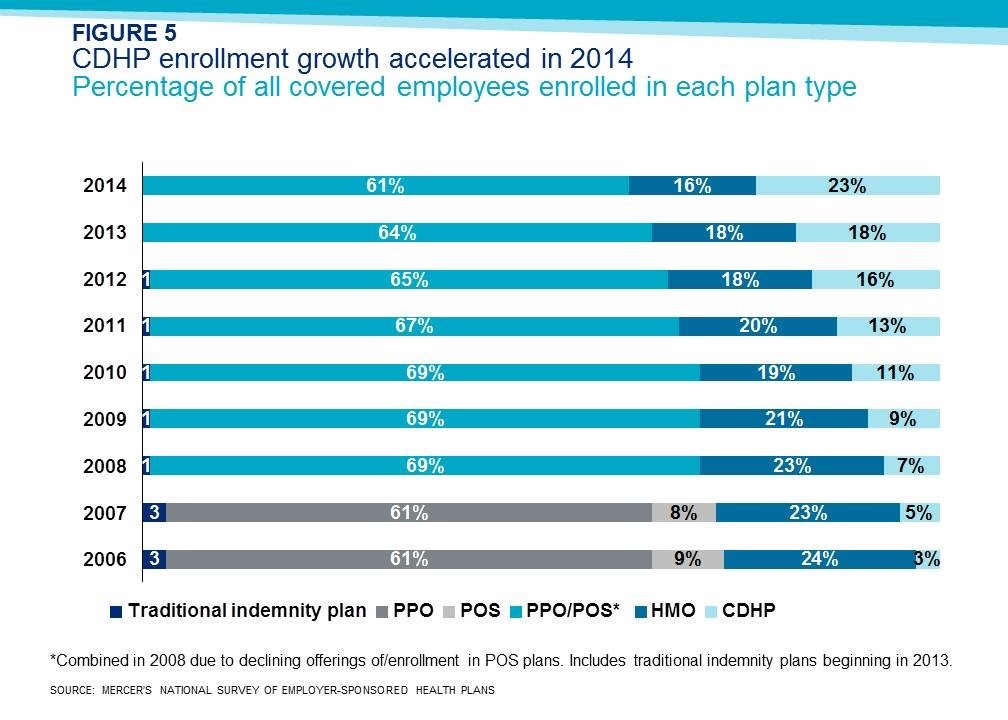
The purpose of such plans is to allow consumers to spend a higher share of their health care dollars directly, instead of through health insurers’ bureaucracies. This should make us more cost-conscious. Critics allege that consumer-driven plans merely shift costs, but this is not the case. According to the NHE data just published, out-of-pocket spending jumped 5.9 percent in 2007, before consumer-driven plans had taken root at all. Out-of-pocket spending grew hardly at all in 2008 through 2010, after which it grew at a moderate 3.6 percent in both 2011 and 2012. It grew only 3.2 percent in 2013, slower than the rate of Medicare spending that the actuaries cheer.
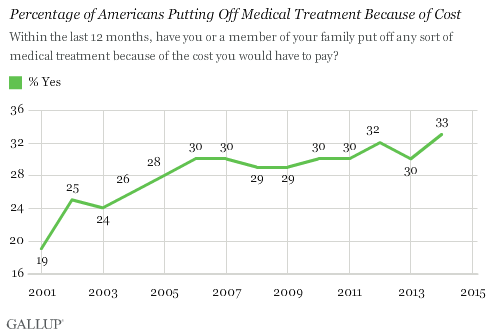
And yet critics complain that this imposes a hardship on patients. Not true: Gallup reports that more Americans are delaying medical care because of cost. It is now 33 percent of respondents, versus only 19 percent in 2001. However, this increase happened between 2001 and 2006, before there were any consumer-driven plans to speak of. Since then, the share of Americans delaying medical care because of cost has bounced between 29 percent and 33 percent.
That figure is likely creeping up because of Obamacare. Remarkably, the increase has almost entirely happened among insured Americans with middle-class and higher incomes. About 34 percent of privately insured respondents reported that they had delayed medical care due to cost in 2014, versus only 25 percent last year. About 28 percent of respondents in households with incomes of at least $75,000 reported delaying treatment, versus 17 percent in 2013.
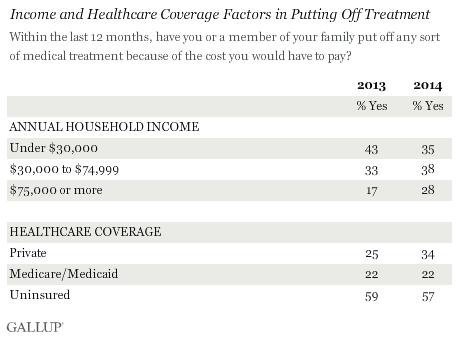
The confusing figure in the Gallup poll is the proportion of respondents with household incomes under $30,000 who delayed treatment due to cost, which dropped from 43 percent to 35 percent. It appears that the drop is among healthy people who signed up for heavily subsidized Obamacare exchange plans and took advantage of “free” preventive care. We know that very sick people have extremely high out-of-pocket costs under Obamacare.
Obamacare is likely having no effect on health spending. Its most measureable consequence is to significantly increase financial hardship among middle-income and high-income voters. It’s no wonder Democrats like Senator Chuck Schumer are jumping off the bandwagon.


Can anyone tell me whether the MLR is based on paid or incurred claims? If incurred, setting claim reserves is as much art as science and allows for earnings smoothing over years. Excess reserves from one year will be released in a subsequent year, and vice versa.
One perverse incentive of the MLR is that fraudulent claims paid are considered medical costs, whereas money spent in an effort to avoid paying fraudulent claims is an administrative expense.
John, I knew that you would be burning the midnight oil coming up with any reasons you could divine to not give the ACA any credit for the continued health care spending slowdown. I am also not supprised that the Repubs would also start taking credit for Obama’s sequestration if it turned positive. [“… and the Republican-driven sequestration also held back spending.”] I personally applaud Obama’s sequestration. If Congress cannot cut the sacred cows out of the herd themselves, then Big O has to do their work for them again. Also, as evidenced by the slowdown, if the health care industry could not control themselves and reign in their double digit increases per year, the resultant ACA legislation was the proper prescription.
While I was burning that midnight oil, the lamp tipped over and I got a burn. I am still looking for the ICD-10 code for that.
@Al
The reason I cannot give the PPACA credit for the health care spending slow down is because there is no reason within the framework of economics to support the idea. There is, however, economic theory to support the argument that high-deductible health plans and the lingering recession have slowed spending growth. You could even argue the patent cliff that has slowed drug spending may have helped moderate the growth in health expenditures. The CBO doesn’t believe ACOs have had any widespread desirable effect on costs. Boosting coverage and boosting Medicaid enrollment certainly would not be associated with a slowdown in spending.
So who’s better at standing on his head, Graham or Herrick?
Happily we don’t need to know now. The way things are going, both will have years of further opportunities to display their down-is-up, black-is-white, conservative-think-tank-spawned-ACA-is-now-the-worst-thing-on-planet-earth dissimulation skills.
I help a couple of neighbors with their Medicare. Both have chronic conditions requiring more frequent attention. Medicare is often denying claims which generally leaves the provider eating the cost. I help them appeal their denials but sooner or later, those providers will not entertain Medicare recipients, or will entertain them only with agreements to pay if Medicare denies.