Health IT to Raise Costs, and Other Links
73% of doctors: Health IT will raise quality; 71%: it will also raise costs.
The highest paid public employee in your state is… [HT: Jason Shafrin]
This is what happens when the government ignores Dr. Jeffrey Brenner:
For more than two decades, Wanda Remo has battled one illness after another. Asthma, chronic lung disease, heart disease, high blood pressure, arthritis, depression, chronic pain, strokes. Specialists treat her lungs, her heart and her joints.
Her litany of ailments brought her to emergency rooms six times last year, between numerous additional visits to a federally subsidized health clinic in South Los Angeles.
“You are one of the million-dollar patients,” her doctor, Derrick Butler, tells the 57-year-old as she leans on her walker during one appointment. (LA Times)
In 25 years Medicare spending is projected to reach one-quarter of all federal expenditures, about 6 percent of gross domestic product (GDP). Several proposals to reduce the growth of Medicare expenditures have been debated in recent years. These include:
1) Mean-tested premiums for Medicare Part A Hospitalization.
2) Premium support, providing seniors a credit to purchase private plans.
3) Raising the Medicare eligibility age to 67.
Means testing Medicare Part A premiums only reduces Medicare expenditures by 2.4 percent through 2037. Increasing the age of Medicare eligibility to age 67 reduces the cost by three times that amount — 7.2 percent. The proposal with the most potential was premium support. If a tax credit was tied to the growth in the economy, the savings is equal to 5.4 percent. However, if the premiums credit was tied to the consumer price index (i.e. merely adjusting for inflation), the program would save 24 percent.
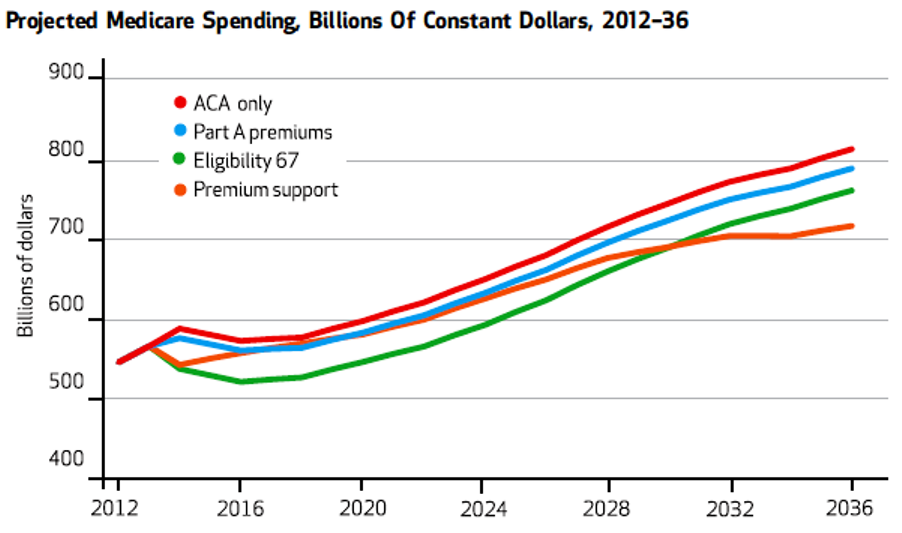
Source: Health Affairs.
A version of this Health Alert (co-authored by Pamela Villarreal) appeared at Townhall.
One of the worst features of the American health care system is the sorry state of medical malpractice law. Fewer than 2 percent of injured patients ever file a lawsuit. Of those that do, only one in 15 receives compensation. More than half of every dollar goes to cover the cost of litigation, rather than to the injured and their families.
Ironically, the medical malpractice system is inordinately focused on whether someone was at fault when an injury or accident occurs. Of the estimated 187,000 deaths (NCPA estimate based on NEJM and NCBI) and 6 million injuries that occur in hospitals each year, only an estimated one in four are considered negligent (malpractice) — and the actual number is probably much lower than that. Another 30 percent (such as certain types of infections) are judged to be “preventable,” even though no one is guilty of negligence. Almost half of adverse medical events are “acts of God” — no one was at fault and there is no obvious way of preventing them.
In Bensonhurst, Brooklyn, at the new R&G Social Adult Day Care Center, known locally among elderly immigrants for luring clients with cash and grocery vouchers, most people there for lunch did not stay to eat. Instead, many walked briskly toward the subway carrying bags stuffed with takeout containers, and two elderly men rode away on bicycles with the free food.
Not a wheelchair or walker was in sight at these so-called social adult day care centers. Yet the cost of attendance was indirectly being paid by Medicaid, under Gov. Andrew M. Cuomo‘s sweeping redesign of $2 billion in spending on long-term care meant for the impaired elderly and those with disabilities.
Such centers have mushroomed, from storefronts and basements to a new development in the Bronx that recently figured in a corruption scandal. With little regulation and less oversight, they grew in two years from eight tiny programs for people with dementia to at least 192 businesses across the city.
Next time you hear someone say how we need to replace fee-for-service payment with bundled payments plus managed care, pull out this article from the NYT. Matt Yglesias comments.
A common starting point is the assertion that those who are obese impose higher health costs on the rest of the population — a statement which is then taken to justify public policy interventions…We will argue that the existing literature on these topics suggests that obese people on average do bear the costs and benefits of their eating and exercise habits. We begin by estimating the lifetime costs of obesity. We then discuss the extent to which private health insurance pools together obese and thin, whether health insurance causes obesity, and whether being fat might actually cause positive externalities for those who are not obese. If public policy to reduce obesity is not justified on the grounds of external costs imposed on others, then the remaining potential justification would need to be on the basis of helping people to address problems of ignorance or self-control that lead to obesity…
Oops. There goes the whole reason for Mayor Bloomberg’s soda ban and his call for a soda tax. The study. HT: Jason Shafrin.
Traditionally, insurers are liable for processing a claim regardless of whether a consumer has paid his or her premiums. However, the ACA allows insurance plans offered through the exchanges to delay paying the claims of consumers who have failed to pay their premiums for two months and to deny all claims for beneficiaries who have not paid for three months. As a result, physicians who want reimbursement from such consumers will have to recoup their expenses directly from the patient…the claims of beneficiaries who have not paid their premiums might create a “dramatic financial challeng[e]” for physicians and potentially exacerbate a physician shortage, MedPage Today reports.
If every vendor in the world (from gas stations to taxicab drivers) can verify a credit card in a matter of seconds, why can’t doctors verify whether an insurance card is valid?
It turns out that the costs of the Affordable Care Act — ObamaCare to its unyielding Republican foes — are sprinkled here and there through hundreds of pages of budget books. It’s partly due to the arcane ways of government budgeting. It may also be an effort to avoid giving foes more of a target.
“I’m sure somebody has a spreadsheet somewhere, but clearly they are not publishing it in this budget,” said Bill Hoagland, senior vice president at the Bipartisan Policy Center. “There is a political aspect to this and there is literally a green-eyeshade part. Once you have adopted a policy it’s difficult to just pull it out.”
More in The Washington Post.

