Divergence in Private Versus Public Health Facilities Construction Continues in September
 Construction of health facilities slowed in September, along with other construction. Overall, health facilities construction starts declined 0.3 percent in September, versus a drop of 0.4 percent for other construction. Health facilities construction accounted for 6 percent of non-residential construction starts. However, the divergence between private and public continued.
Construction of health facilities slowed in September, along with other construction. Overall, health facilities construction starts declined 0.3 percent in September, versus a drop of 0.4 percent for other construction. Health facilities construction accounted for 6 percent of non-residential construction starts. However, the divergence between private and public continued.
Construction of private health facilities dropped 1.0 percent, versus a drop of 0.2 percent for other private construction. Private health facilities construction starts accounted for almost 8 percent of private nonresidential construction starts. Construction of public health facilities increased a whopping 2.4 percent, versus a drop of 1.0 percent for other public construction. Is this what they mean by “infrastructure” spending – broken bridges and roads, while more VA and county hospitals spring up?
(See Table I below the fold.)
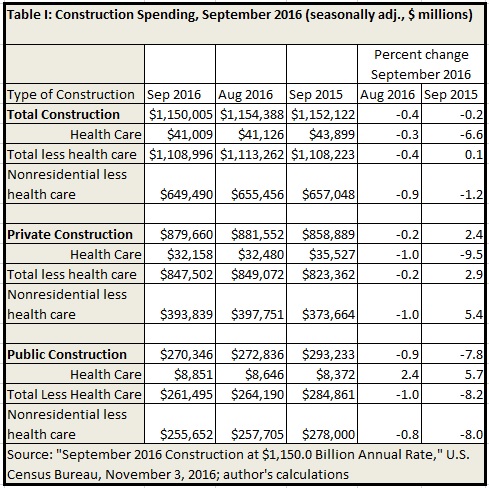
For the twelve months ending last September, there is a significant difference in trend between private and public construction. Non-health private construction increased 5.4 percent, but private health facilities construction dropped 9.5 percent. On the other hand, non-health facilities public construction dropped 8.2 percent, but public health facilities construction increased by 5.7 percent.
Overall, health construction dropped 6.6 percent, versus an increase of 0.1 percent for non-health construction. If the divergence between private and public health facilities construction persists, it will suggest investors expect VA, Medicaid, “uncompensated” care to grow as a share of U.S. health spending, versus private payment.

