Is Consumer-Driven Health Care Hurting Hospitals? (And Should We Care?)
Dobson DaVanzo, a leading consulting firm, has produced a report for the Federation of American Hospitals, the trade association for for-profit hospitals. The report notes that the rate of change of health spending has slowed down. Indeed, the report concludes that spending is set to shrink this year by over one percent. This introduces a “paradox”:
However, paradoxically, consumers perceive that their health care spending is increasing more than usual. This perception is largely a result of spending on their health care increasing faster than personal income combined with a continuing redesign of their health insurance benefits, which shifts more of the cost burden onto consumers:
- Almost 60% of Americans think that health care costs have been growing faster than usual in recent years, and more than 70% of consumers attribute responsibility for their perceived high and rising costs to health insurance companies.
- Total premiums have increased substantially over the past decade, from 14.9% to 21.6% of median household income between 2003 and 2012.
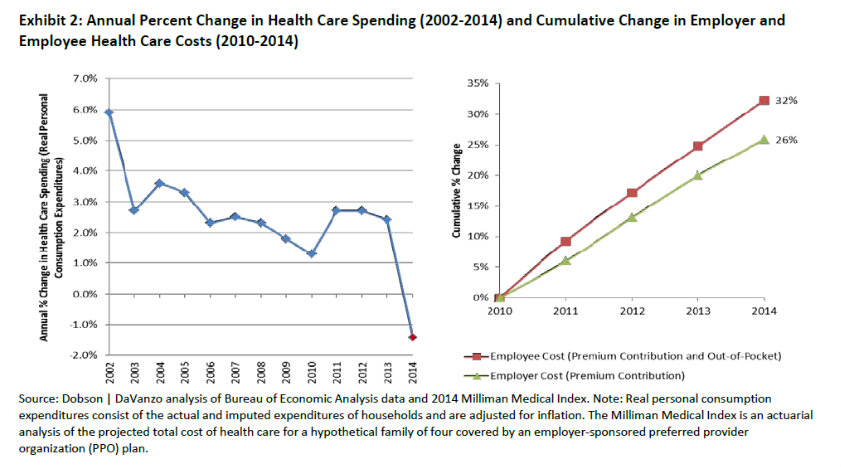
- Employee contributions to premiums and out-of-pocket spending have risen 23% faster than employee costs since 2009 (32% in cumulative growth vs. 26%) (See Exhibit 2).
Read More » »