Magical MAGI: Defining Who Gets ObamaCare Subsidies
A person who buys an ObamaCare health insurance policy can get a tax credit (subsidy) if his household’s Modified Adjusted Gross Income (MAGI) puts him below 400 percent of the Federal Poverty Level (FPL).
But what is a household?
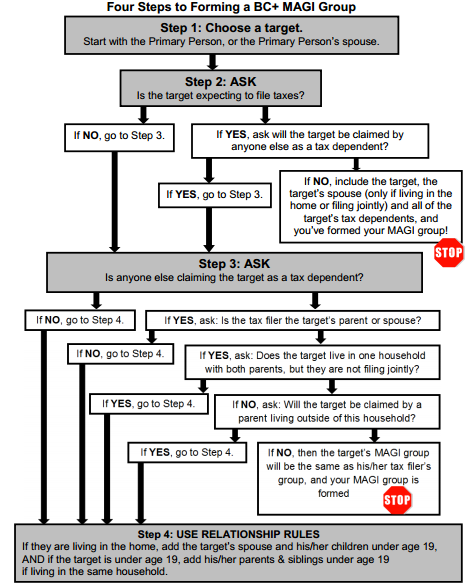
It isn’t easy figuring out those magical MAGI groups when ObamaCare premium subsidies depend on family size and the definition of a family is, shall we say, rather flexible. As the Wisconsin training handout puts it, “the new MAGI methodology introduces tax relationships into the way we build BC+ [BadgerCare Plus] household composition. Under MAGI, household composition is formed using either ‘tax rules’ or ‘relationship rules.’ The use of tax rules versus relationship rules is based on whether or not the individual for whom the assistance group is being formed intends to file taxes or is a tax dependent.”
The manual goes on to say that it is important to remember that because Assistance Groups are person specific, “the household composition for each Assistance Group must be examined one person at a time and each Assistance Group is formed around a target (the individual who is requesting assistance). The target’s assistance group is formed based on that target’s age, marital status, tax filing status, tax relationships and/or family relationships.”
If you have a “target” living in a spare room or basement, here’s a flowchart that might come in handy: