The Future of Medicine and the Internet of Things
As previously noted on this blog, investments in digital health ventures doubled in 2014. Institutions, analysts and MDs envision the opportunity to reduce the colossal inefficiency of current medical practice by exploiting the Internet of Things.
According to a recent JAMA article, the number of mobile devices connected via the internet is doubling every five years, and there will be nearly seven connected devices per individual by 2020.
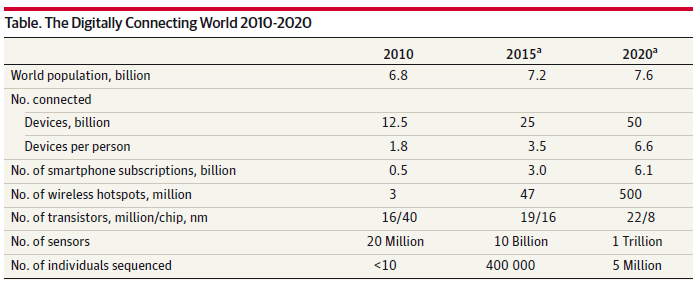
Source: Digital Medical Tools and Sensors from JAMA.
Read More » »