Healthcare Prices Flummox the Experts
The absurdity of our healthcare pricing is never more clear than when described by experts — people who study the system for a living — who become patients and are shocked and confused by the bills that hit them. Here are three examples:
1. Paul Keckley, PhD, is one of the top consultants in the healthcare sector. From 2006 to 2013, he ran the Deloitte Center for Health Solutions, a period during which it rose to prominence and produced excellent research. Well, Mr. Keckley has just undergone knee-replacement surgery:
This week, I started getting the bills: the whopper $51,829.35 from the hospital for my 55-hour stay. And that doesn’t include professional fees for my surgeon, internist and anesthetist, the 3 medications I now take, the crutches and walker I bought, and the over-the-counter aids I’ve purchased. In all likelihood, the final tally will be close to $60,000. Wow.
I don’t know how to place a value on walking with confidence and without pain. I took the plunge hoping for the best and oblivious to costs. I studied report cards about my surgeon’s performance and infection rates for the hospital we used. I tried, to no avail, to estimate costs, and investigated out-of-market options for a bundled package. In the end, my local option was best, but there were more unknowns than knowns as I went under the knife.
At the bottom of my bill, the hospital noted “We have filed a claim with your insurance carrier. Please take a moment to review the insurance information listed above in order to ensure your claim is billed accurately.” It’s nice of them to forward the bill to the insurance company, but I’d like to sign off on what was charged before it’s sent, and I don’t have a clue what some of the 11 items even mean. What’s the “central service” and “PASR”, and why was there a separate billing for the “laser surgery center,” that’s different, I guess, than the “operating room” charge of $38,092.80. But I intend to find out, and notify both my insurer and providers what I learn.
2. Veronica Combs is Editor-in-Chief of MedCityNews, a source of excellent coverage of innovation in healthcare. Here’s her story of her CT scan:
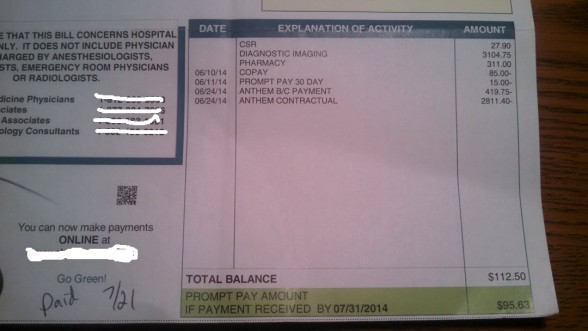
I had a CT scan in early June. This is the bill for it. Here is how I read these numbers:
- List price for the scan: $3,104.00
- Anthem’s evaluation of what the scan is really worth: $419.75
- Hospital’s padding: $2,811.40
Also, I like — but am puzzled by — the prompt payment discount. This tells me that hospitals can work like other service businesses that give discounts to customers who pay quickly. It also tells me that the scan is not even worth the $419.75 that Anthem forked over…
What is a fair price to pay for a CT scan? I imagine Anthem’s set reimbursement is stingy. I would pay more for the service because it was a good one and because of the additional safety factor of the dose-adjusting software.
But what is a fair price? I don’t have the time to call around and price shop. And people who have taken the time to do so have been frustrated by bureaucracy and hospitals’ inability to calculate a price.
I have the resources to pay my bills and I want to pay them. I also want to understand what I am paying for and what the services are actually worth. I have been tempted several times to offer to pay a cash price for healthcare services, even though I have insurance. It would cut down on so much frustration and hassle and faxing. I haven’t gone there yet, but this minute clinic vs. hospital experience was a big nudge in that direction.
3. Finally: Yours truly. My family doctor scheduled me for a hospital procedure in September, so I haven’t seen any bill yet. I called my insurer and the hospital, and both assure me the procedure is preventive, so I won’t have any co-pay. We will see. More interesting was the hospital telling me I have to get a prescription filled before the procedure, and asking me which pharmacy I use. Well, I don’t, because I don’t take any prescriptions. But there is a pharmacy by the office where I buy my over-the-counter medicine, so I looked up its address and gave it to the hospital. The hospital said the retail pharmacy would have the prescription later that day. I walked in the next day and presented myself to the pharmacist, telling her that I’d never been there before but that she had a prescription for me. I was sure she’d look at me like I had two heads — neither functioning properly — but my name and birthday was all she needed to find the prescription. With my insurance, the co-pay was $10 instead of $25.
So, there you have it: Three stories. Two describe a system that is not changing at all. The third describes one point in the system — e-prescribing — where change is well underway. Pharmacies, of course, are where convenient clinics, with transparent prices, are opening up. So, if you were to ask me where the most exciting changes in healthcare will be happening over the next few years, I’d say it may be in retail pharmacies.


The price most relevant to patients with insurance is the insurer’s actual contract reimbursement rate, not the provider’s full list price or chargemaster rate in the case of hospitals. Since both insurers and providers are precluded from disclosing contract payment rates by confidentiality agreements, accurate price shopping and price determination before services are rendered is, for all practical purposes, impossible. Eliminating these confidentiality agreements either by regulators or legislators would go a long way toward allowing both price discovery at a particular provider and price shopping among providers. List prices are irrelevant in this context except for the uninsured and for patients contemplating using an out-of-network provider.
In the case of prescription drugs, at least patients can learn what their copay is and what the drug’s retail price is before the prescription is filled and paid for by calling the pharmacy. The patient can also determine whether or not it’s on the insurer’s drug formulary, and, if so in what tier.
As for the right or fair price for an MRI, I think it should be based on the amount of machine and staff time required to complete the test. MRI machines are expensive and need to be in operation for a reasonable number of hours per day or per week to cover costs, including the cost of capital. The same principal is used by paper mills which is also a capital intensive business. The amount of machine time required to produce the customer’s order is a key part in determining how much to charge for a given order.
“List prices are irrelevant in this context except for the uninsured and for patients contemplating using an out-of-network provider.”
It’s kind of like buying a car, no? Unfortunately, care shopping is usually a fun affair, while shopping for health care is not so much.
We find MRI costs in our area are usually much higher for hospital based imaging centers than private ones.
Shopping around for medical procedures aren’t going to be enjoyable like buying a car until they can install a Bluetooth in me!
“So, if you were to ask me where the most exciting changes in healthcare will be happening over the next few years, I’d say it may be in retail pharmacies.”
Yes, perhaps for the consumers. But pharmacists may tell you a different story, as staffing has become more difficult and full time pharmacist positions in retail are becoming a thing of the past.
How can the lack of transparency and consistency of healthcare prices still exist in a country currently under massive healthcare reform. If healthcare prices are flummoxing the experts, its going to flummox the rest of us too!
It’s debatable that there’s actually reform going on.
“But what is a fair price? I don’t have the time to call around and price shop. And people who have taken the time to do so have been frustrated by bureaucracy and hospitals’ inability to calculate a price.”
There needs to be a push to increase healthcare price transparency. People very seldom have the time to shop around for personal goods, much less their health care. If Obamacare wanted to take a step in the right direction for once, they would address the issue with opaque prices.
But people do shop for personal goods. Price transparency is such that they are able to swing by Kroger’s on the way home and have a good idea before we even get there what to expect. For something like a flat screen TV, consumers may shop a little more. A procedures like a CT scan has the potential to cost as little as a medium sized, store brand flat screen TV, or as much as a name brand 72″. If you were shopping for a TV, you pay more attention to the price, quality and size. It makes sense for patients to do the same or suffer the consequences.
Veronica Combs at MedCityNew has a story similar to a friend of mine. She went to a hospital to have a CT scan done and found out she would be out something like $2700 — even with the Blue Cross negotiated discount. I looked online and quickly found a facility nearby that only charged $435 with her Blue Cross discount. She had had some lab work done at the hospital and was very angry to discover they wanted $700 for a service that should have cost $200 elsewhere. Oddly enough, a bill collector called wanting payment and she informed him she had never received an invoice. When she asked for one, he couldn’t produce one. Something as simple as producing an invoice to show her what she was paying for is like pulling teeth. As a result, she’s in no hurry to pay them.
Exactly. I knew a person who “mis”represented himself as uninsured and got a cash price from a hospital for an outpatient procedure. I can’t remember what it was. Let’s say $2,000.
He was admitted with his insurance and after the fact, his EOB said that he owed $4,000 and the insurer paid $2,500, for a total of $6,500.
When he got the invoice from the hospital, he mailed it back – unpaid – with the quote for the cash price. He noted that the insurer had already paid more than the cash price, so he declined to pay the co-pay.
That’s the last he heard of it.
Insurers want to move providers away from the fee for service payment model and into value based contracts that will require them to assume some financial risk. If they want doctors to know and to care about costs as part of their job, they will have to make it much easier for the docs to see what actual contract reimbursement rates are for all providers in the region in real time. There will also need to be credible quality information for more complex procedures like heart surgery and the information will need to be easily accessible and user friendly.
Today, hospital prices can easily vary by a 500% or more even in the same city with no discernible difference in quality. If we want medical prices to converge to a reasonable level not too far above Medicare rates, we will need real price and quality transparency for both doctors and patients. For more expensive procedures, medical tourism, at least within the U.S., also needs to be a viable option.
The hospital or MRI center charge means nothing. It’s the insurance allowable rate that is what’s contracted and thus payable to the hospital. Quibble about that, not the “suggested sticker price” as the new car analogy exemplifies.
Note to Devon:
Veronica C needs more legal protection than just refusing to pay the bill. The unpaid bill could easily damage her credit.
I go back to my old ideas:
a. either health courts, which would have binding authority to reduce or toss out extortionate bills;
or
b. all-payer regulation.
As I noted in an earlier exchange with Barry, the greedy hospitals might accept solution (b), if the alternative was endless hearings through my solution (a).
For Mr Keckley’s knee surgery and its ludicrous bill, the solution is this:
a. compute how much hospitals need to survive, based on the days of care they would provide if they were two thirds full, and if they paid no astronomical salaries to anyone.
This is not rocket science. The amount might come to $3,000.
b. They then receive $3,000 a day.
The bloated bills for surgeries would disappear.
The above procedure is approximately how Germany controlled costs in the late 20th century, as documented by Joseph White in Competing Solutions.
Bob,
I once heard a presentation by an expert on the German healthcare system at a conference. She said that when hospitals were paid on a per diem basis for all or most care, they would often admit patients on a Friday so they could get paid for the weekend days when very little happened except for emergencies. Care was generally slow-walked following surgery so people spent more time in the hospital than necessary before being discharged again so they could get paid for days when the patient needed little more than rest. Average length of stay is shorter in the U.S. than any other country, I believe. I think she said that Germany ultimately adopted a version of Medicare’s DRG (case rate) prospective payment system.
CMS already requires hospitals to provide it with cost reports. I think hospitals should be required to indicate on every bill what its charges are as a percentage of the Medicare allowance which, by the way, is not shrouded in secrecy by confidentiality agreements. For academic medical centers and safety net hospitals, the Medicare allowance should exclude the payments they receive from separate CMS budgets for direct and indirect medical education and for disproportionate share payments.
As I’ve said many times before, the uninsured and patients who find themselves out-of-network should be charged no more than 115% of Medicare and, for services, tests and procedures that Medicare pays at least $500, bills above 150% of the Medicare allowance should be viewed as unreasonable on its face.
Thanks Barry. i think we are both circling around the same flame.
So far the big difference is that Germany had the political strength (or whatever)
to impose DRG pricing on all hospitals. For that to happen in America, it will I think require a remarkably thick-skinned administration. I cannot see Congress imposing anything which cuts off their existing campaign contributions from hospitals.
Bob,
Maryland uses an all payer system which dates back to 1977. It only applies to hospital based care with allowable prices set by the Healthcare Services Cost Review Commission (HSCRC). It hasn’t reduced medical cost growth in MD as far as I know but it does prevent certain patients, especially the uninsured, from being gouged. There are also weird games that are played. For example, if a hospital builds a new imaging center in a separate building on its main campus, it’s considered “unregulated space.” So, you have the spectacle of an inpatient being transported 200 or 300 yards by ambulance from the main hospital to the on campus imaging center so he can get his test which is then billed under unregulated rules.
At any rate, to replicate MD’s system across other states would require Medicare and, especially, Medicaid to pay significantly more than they do now so private insurers can pay less. Given the federal fiscal situation and the fact that Medicaid is already the largest or second largest budget category in most states, it’s unlikely to happen.
As for Germany, their system uses insurance companies, albeit nonprofits, called sickness funds. There is no Medicaid for the poor or Medicare for the elderly. Insurers and providers both negotiate as a group or consortium to set rates for all services, tests, and procedures in each region. We would need an anti-trust exemption for insurers and providers to adopt that approach in the U.S. and the larger insurers and probably hospitals would resist it because they believe they get a better deal than their smaller competitors under the current system. Drug prices and drug formularies are negotiated at the federal level in Germany, I believe.
I think just getting rid of the confidentiality agreements that preclude disclosure of contract reimbursement rates would go a long way toward bringing about pricing convergence at least for commercial insurance though those rates would still be well above Medicaid and somewhat above Medicare on average. Insurers’ interest in moving away from the fee for service payment model in favor of value based contracts plus reference pricing and bundled payments where appropriate, coupled with the proliferation of high deductible health plans and tiered and narrow insurance networks will all move the system in the right direction over time. There do need to be special protections, though for the uninsured and for patients who find themselves out of network when receiving care that must be delivered under emergency conditions.
As for the single payer model, keep an eye on Vermont. Coming up with a viable financing model will be a huge challenge. Vermont has the advantage of small size with a population of 600,000 and only seven hospitals spread across the state or eight if you count Dartmouth-Hitchcock just across the border in New Hampshire. Even in VT, though, Medicare and Medicaid would continue as would the VA system and out-of-state self-insured companies with employees in VT could maintain their existing commercial insurance as well.
Oh, yes: We will be keeping an eye on Vermont. Fear not! Maybe they’ll be exporting patients to Montreal!