Medicare by the Numbers
Here are the five most important things you need to know about Paul Ryan, Barack Obama and Medicare. You won’t find this anywhere else.
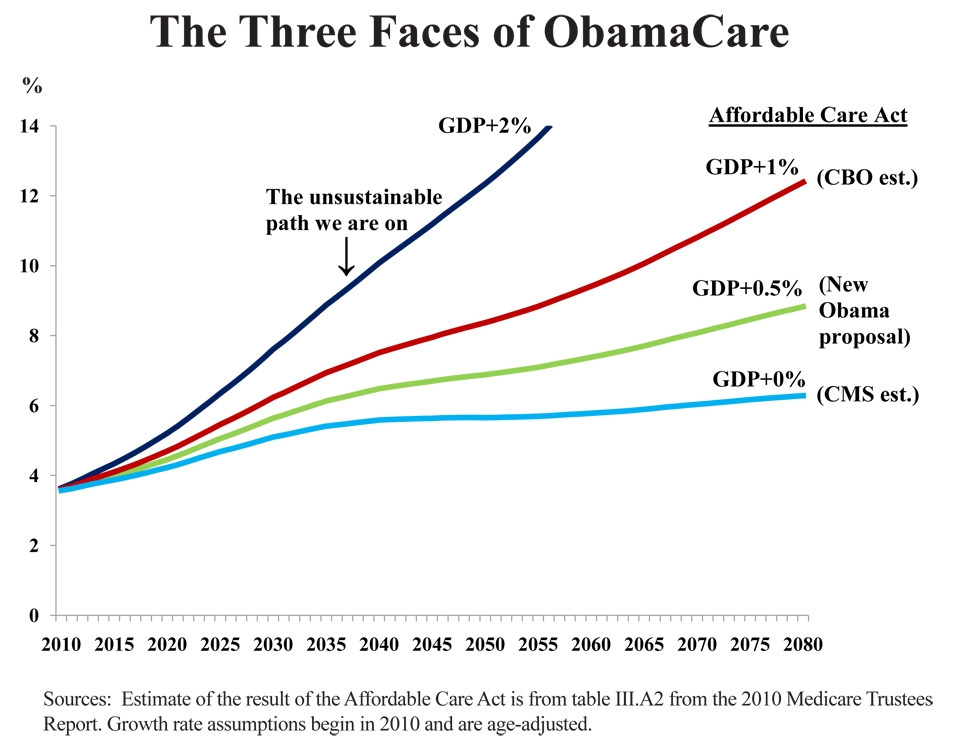
1. Seniors Take It on the Shin. Without any help from Paul Ryan — and without a single Republican vote — the Affordable Care Act is going to reduce spending on Medicare by $523 billion over the next 10 years, relative to what it would have been. This reduced spending — which will mainly consist of lower fees for doctors and hospitals — will continue into the future and will be enforced by an independent commission. Although the Congressional Budget Office (CBO) and the Centers for Medicare & Medicaid Services (CMS) have different projections, Obama administration representatives have officially signed off on the CMS report, which projects that Medicare will grow no faster than the rate of growth of gross domestic product (GDP), as the following chart shows.
To give you some idea of how radical this change is, on the day Barack Obama signed the Affordable Care Act legislation, he cut Medicare’s long-term, unfunded liability in half!

2. My Line Is Lower than Your Line. Despite the hysteria on the left about the Bowles/Simpson, Rivlin/Ryan and the Domenici/Rivlin plans, the ObamaCare Medicare cuts are much harsher than any of these proposals. And most critics of these entitlement reform plans were enthusiastic supporters of ObamaCare.
Ignoring the political maxim to never get between an opponent’s gun and his foot, the new Paul Ryan budget manages to top even ObamaCare by roughly tracking the Affordable Care Act spending for the next decade and then allowing Medicare spending to grow no faster than the consumer price index.
In response to Ryan, President Obama has proposed a growth rate for Medicare of GDP + 0.5%, which is less than the CBO projection for ObamaCare (GDP + 1%) but more generous than the CMS projection (GDP + 0%), which the administration has already signed off on. Go figure. (See the chart below.)

3. Not Reforming Health Care. None of the proposals (including ObamaCare) have any serious plan to reduce health care spending for the country as a whole. This means that Medicare spending will fall further and further behind what everyone else is spending under every proposal. Under ObamaCare, for example, the Office of the Medicare Actuaries estimates that Medicare payments will fall below Medicaid payments by the end of this decade. Also, none of the proposals have any mechanism that would allow people to build up tax-free savings to be able to afford to replace reduced Medicare spending with personal out-of-pocket spending. This is enormously important because none of the projected cuts will be made if a backlash from elderly voters makes them politically impossible.
4. Ignoring What Has Already Been Proposed. The Coburn/Ryan health bill is the only serious proposal to fundamentally change the economic incentives of employers, employees and medical providers. But even it does not go far enough to bring total health care spending in line with what is being proposed for Medicare. We have suggested ways of making the Rivlin/Ryan plan better and achieving reasonable goals here.
5. Ignoring What Is Already Being Done. Despite the hysteria over the idea of Ryan’s concept of “premium support,” the idea actually originates with left-of-center economists Henry Aaron and Bob Reischauer (see Ezra Klein) and we already have it in Medicare. It’s called Medicare Advantage and about one-fourth of all Medicare enrollees participate in it. In addition, the subsidies for private plans sold in ObamaCare health insurance exchanges will also morph into premium support. We also already have something similar to Accountable Care Organizations (ACOs) — the Obama administration’s hope for controlling costs for Medicare. They are called Medical Service Organizations (MSOs) and they service Medicare Advantage plans — the plans ObamaCare has targeted for defunding. (Again, go figure.) I’ll write about this more in the future.


{kind=link}
Good post. Graphs make everything very clear.
No song pairing this morning? I feel cheated.
Thanks for this post. Nobody else seems to get this.
The grim reality facing everyone over age 65 or those hoping to get to 65 is that both political parties are going to ask them to die sooner than necessary so America can be more globally competitive. Whatever that means. Will the Medicare Independent Payment Board, the PCORI, and the ACOs do the dirty work of rationing, or will it be the traditional managed care Medicare Advantage willing executioners? Both will use “evidence based” algorithms. It will all be very scientific,and equally deadly. Perhaps a re-reading of a bio of Nazi doctor Karl Brandt is in order just to gain some historical persepctive of where all this leads.
The ACA calculations, as we know, were based on reductions in reimbursements that are unlikely to happen. The CMS report cannot be taken seriously either. Ryan is a step in the right direction, good opening dialog. But we almost-Medicare enrollees must agree to delay enrollment (by law), allow MD balanced billing, and means testing. Otherwise, let’s throw in the towel now, and find a new way to govern ourselves, because this one certainly isn’t working anymore.
Brant, than’s a pretty scary picture of the future you are painting.
@ Dave Racer
For the next ten years, Ryan’s budget just follows Obama Care’s cuts in Medicare spending. So if Oba,a Care cuts are unrealistic and won’t happen, neither will Ryan’s.
Premium supports are a step in the right direction. Critics bristle at the thought of seniors having to navigate an Insurance Exchange, comparing benefits and possibly having to dig into their own pockets to pay for benefits beyond the age and risk-adjusted payments.
The top-down approach to controlling spending, espoused by many, is to slash Medicare reimbursements and force providers into large networks where a pot of money is split among stakeholders for meeting conditions that (will probably) have little to do with actually outcomes. Houwever, 50 million seniors can do more to hold the line on spending than a handful of bureaucrats in Washington and Baltimore.
John,
While the Ryan Budget does get rid of the IPAB, it does not get rid of the ACA cuts in hospital and doctors payments. In fact, starting in 2022, there will be less money coming form Medicare to pay for doctors and hospital visits, sicne seniors will have to make up the $ 6,000 difference by buying a supplemental policy to cover what the government subsidy will not pay for. While competition may reduce the $ 6,000 figure, it is clear that many seniors who rely predominately on SS and a small pension will not be able to afford the level of coerage they now have.
Bill
I’m not sure I see the point of the Ryan budget. We have to control Medicare spending, but its not going to work without overall health reform.
From a practical standpoint, can seniors manage all the paperwork and decisions required for managing one’s own health care?
Good analysis, John. Reform must be part of any proposed spending cuts.
Tom
@Tabitha C.
Seniors won’t have to “manage all the paperwork and decisions required for managing their health care”. The paperwork does not “have” to be a big deal. One has to realize what a complicated mess we have made of the health care delivery process. It should not be that much more complicated than paying ones utility or credit card bills if unnecessary red tape is eliminated.
Insofar as making treatment decisions, what is wrong with reliance on the personal counseling that “should” be going on between the physicians and their patients? Are we worried that unscrupulous doctors will take advantage and over treat seniors? Would the extent of that risk not be less than the huge current cost of Medicare fraud foisted on the government and third party payers who are “managing” the program?
Must we make the assumption that people (including seniors) are all so incompetent that they are not capable of doing anything for themselves?
Uwe Reinhardt has a critical analysis of the Ryan plan at the New York Times economics blog today:
http://economix.blogs.nytimes.com/2011/04/18/comparing-ryans-medicare-plan-to-what-congress-gets/
Unfortunately, Uwe makes no mention of how bad ObamaCare is going to be for seniors. I think this is the only blog where you get an objective analysis of both plans.
Thanks for the excellent post. The charts give a really great representative of the impact of different plans.
A philosophical question: Is there any way to cut the budget that will accomplish our two big goals: ensure America’s sustainability and give seniors the care they want? I don’t see any way to avoid cutting benefits and/or more deficit spending. Whatever happens, it won’t be pretty.
@ Virginia
Yes there is a way of doing this. See Framework for Reforming Medicare, avaliable at this site. We need to free the supply and demand sides of the market and we need you people to pre-fund most of their benefts.
@ Frank Timmons
you are right. Almost all the unnecessary paperwork is caused by government regulations — including the incomprehensible hospital bills.
@ William Signer
I think I agree with your main point. Unless there is genuine health care reform, cuts in Medicare spending will largely be shifting costs, not curtailing costs.
@ Brant Mittler
I hope you are wrong, but I fear you are right.
@ Tabitha C.
I agree with Frank’s response to you.
@ Dave Racer
You are right that the Medicare cuts under Obama Care are unlikely to occur, but the same criticism may be made of Ryan’s budget. Again, without fundamental health reform, cuts in Medicare spending will shift costs more than they will cut costs.
@ Tabitha and Frank
In terms of treatment decisions, the answer is
“there is nothing wrong with reliance….”.
The reality: limited time for many physicians to communicate with the elderly and their family. Many of us have had this experience that with our families.
– worries about unscrupulous doctors??? “No”. Most Docs are motivated by their true desire to give the best care they can.
– Extent of risk/cost of Medicare fraud? “Yes”…However, unscrupulous Docs do need to be held accountable…The question is how??
– Assumptions about competence of the elderly….
“Yes”, but not all the time….
Clinicians see this daily from people of all walks of life and age. It’s simply too hard to understand so many details about your health, the personal costs, how to get through the system, the importance of compliance with your meds, etc……
I’m referring to many with PhD’s, MBA’s, college grads too…
I don’t understand the legal system either…
The elderly (and their children) simply don’t like hassling with bills even if it is only 1 bill.
@ Dr. Chris Ewin
“The elderly (and their children) simply don’t like hassling with bills even if it is only 1 bill.”
What you say is certainly accurate Chris. On the other hand, and at the risk of sounding hard, a lot of people don’t like flossing their teeth or getting up a 7:00 AM to go to work but they do it anyway. It seems obvious that there is no other option, because there certainly is no way a disinterested third party is ever going to do the job properly. Isn’t it insane that we consider bankrupting the country instead of risking inconveniencing seniors (or their caregivers)by requiring them to take care of their personal business?
See my article comparing what Obamacare has done to Medicare to Ryan’s proposal, which I argue is superior:
http://spectator.org/archives/2011/04/13/death-trap-democrats/1
-Peter
Frank,
“Isn’t it insane that we consider bankrupting the country instead of risking inconveniencing seniors (or their caregivers)by requiring them to take care of their personal business?”
I completely agree…
“It seems obvious that there is no other option, because there certainly is no way a disinterested third party is ever going to do the job properly”
I think you’re referring to the elderly and their children paying 1 bill. That is why the fee for care model is working so well….
There is only one bill for the whole year…
@Chris Ewin
“I think you’re referring to the elderly and their children paying 1 bill. That is why the fee for care model is working so well….
There is only one bill for the whole year”
Exactly. But there are all manner of other models that could be successful as well (some yet to be devised), depending upon the preferences of the patients and their doctors. The workable model to encourage this is incredibly simple, and aside from some type of government financial support, why should Medicare/Medicaid not work under the same premise as non M/M?
The key is to use insurance properly (as insurance and not pre-paid healthcare), and get the third party managers out of the equation. It is beyond me why we don’t pound this basic approach in the public arena and make the other side raise specific objections instead of confining ourselves to criticizing the AHCA.
Medicare has been cutting or at least freezing many of its fees for the last fifteen years, and yet its overall spending continues to grow and grow.
A major reason is upcoding. If a medical provider can make twice as much money by assigning a complex diagnosis to the patient, they will do so. In fact there is a large consulting industry which shows hospitals and clinics precisely how to do this.
George Halvorson wrote a still-wonderful book called Strong Medicine in 1996, wherein he quoted one hospital administrator as saying that “We can get around any new fee schedule in about six months.”
If we truly intend to control Medicare spending, we should rip out the entire graduated fee schedule. For example — and this is a very rough proposal –hospitals would get a flat per-diem payment whether the patient had a broken leg or cancer or a heart attack or pneumonia –i.e. $2000 a day, maximum six days, no matter what. Anyone who needed weeks of hospital care could be transferred to a VA facility that the government is already paying for.
This would be a tremendous revenue shock, of course, for hospitals that have invested heavily in recruiting heart surgeons and in buying heart-surgery equipment.
Well, if and when the federal government goes broke, that is kind of too bad.
There was not a lot of sympathy 30 years ago for farmers who went deep into debt expecting certain federal crop subsidies to last forever.
Essentially I am backing up any previous posters who are skeptical that either the ACA or the Rivlin-Ryan budgets will really work. Neither is tough enough.
The nations which actually do cut health costs tend to have large professional bureaucracies, who actively dislike drug companies, hospital chains, and medical entrepreneurs. They also have publicly funded elections, which results in politicians who can afford to alienate potential contributors. America has neither — let’s see what we can do.
Bob Hertz
Director, The Health Care Crusade
Well-said and Excellent points….
Transparent pricing….
But why not keep them out of the hospital in the first place. Concierge models are present that decrease hospitalization rates by 65%……
Primary care
Early access to primary care is the key instead of waiting until a minor problem becomes a big one.
Hello there, I discovered your web site via Google at the same time as looking for a comparable subject, your site came up, it seems to be great. I have bookmarked to my favourites|added to my bookmarks.
I simply couldn’t leave your site before suggesting that I really loved the usual information an individual provide in your visitors? Is going to be again frequently in order to inspect new posts
@ Chris Ewin
You are a crook and evil man, you should not be allowed to speak of patients like you care about them. you would skin a person alive if it increased your bank account. you claim to be a man of god but that is only for your own self centered ego. THERE IS A SPECIAL PLACE IN HELL FOR PEOPLE LIKE YOU. we could ask any of your patients (or cash cows) how they feel about you and they will all say the same thing that you are a bad person and should have your privilege of being a “doctor” revoked!