Headlines I Wish I Hadn’t Seen
Florida Medicare Advantage Plan to pay for members’ fitness trackers (which means the plan seeks to enroll healthy, not chronically ill, seniors).
Florida Medicare Advantage Plan to pay for members’ fitness trackers (which means the plan seeks to enroll healthy, not chronically ill, seniors).
Surgery center of Oklahoma eliminates the $100 aspirin.
Curious factoid: About 20 percent of hospice patients are discharged alive.
Is there anything wrong with distinguishing between the “deserving” and the “undeserving” poor?
Creative destruction: Closed New Jersey hospitals reopen as for-profit medical complexes.
I recently wrote an article critical of a business groups’ approach to improving transparency of prices for medical and hospital procedures. However, we do have a serious problem when it comes to figuring out how much we owe for treatment.
 In Saturday’s New York Times, the estimable Elisabeth Rosenthal has another excellent report (gated, for subscribers only) about a failure in American health care: Even insured patients cannot get prices from their healthcare providers.
In Saturday’s New York Times, the estimable Elisabeth Rosenthal has another excellent report (gated, for subscribers only) about a failure in American health care: Even insured patients cannot get prices from their healthcare providers.
Rosenthal writes about a woman who went to a dermatologist’s office, where a physician’s assistant cautioned her that a white spot might be cancerous. A biopsy confirmed it. Rosenthal then unfolds a “daylong medical odyssey several weeks later, through different private offices on the manicured campus at the Baptist Health Medical Center that involved a dermatologist, an anesthesiologist and an ophthalmologist who practices plastic surgery. It generated bills of more than $25,000.”
The patient’s share was $4,590, which she whittled down to $3,000 after much effort. A highly educated patient, at no point was she told how much her bills would be, nor given an adequate response to her requests for simpler and less expensive treatment. “I felt like a hostage”, she laments.
 Tyler Cowen reviews the literature: the minimum wage does little to reduce poverty.
Tyler Cowen reviews the literature: the minimum wage does little to reduce poverty.
Margaret Carlson’s tribute to Tom Coburn.
CNS News interviews me on “death spirals.”
Bryan Caplan explains why economists put so high an economic value on life.
In Europe, immigrants can move to the country that pays the highest welfare benefits.
I’ve written about sky-high hospital prices in this blog, especially for uninsured patients who present at emergency rooms. A related issue is price transparency. In most normal transactions, it is not hard to discover the price you will pay for a good or service. Indeed, for most ordinary items, prices are posted and we do not even spend much time negotiating.
For much of health care, this is untrue. It is usually very difficult to learn the price of a service from a doctors’ office or a hospital before receiving treatment. Doctors and hospital managers will often reply that they don’t know what the right prices are either, because charges are subject to adjudication by insurers.
When uninsured (and, increasingly, insured) patients are shocked by bills they receive after treatment, they often balk at paying inflated charges. This results in bad accounts receivable for hospitals, which I have argued is a necessary pain to cause hospitals to change.
While everyone outside the health sector agrees that more price transparency would be beneficial, others often propose solutions that increase government regulation. One example is a recent report written by the Pacific Business Group on Health (PBGH), a group of large employers in Northern California.
A year old story that’s worth revisiting:
The so-called bodega clinicas that line the streets of Los Angeles’ immigrant neighborhoods blend into a dense forest of commerce. Wedged between money order kiosks and pawn shops, these storefront doctors’ offices treat ailments for cash: a doctor’s visit is $20 to $40, a podiatry exam is $120 and at one bustling clinica, a colonoscopy is advertised on an erasable white board for $700.
 County health officials describe the clinicas as a parallel health care system, servicing a vast number of uninsured Latino residents, yet the officials say they have little understanding of who owns and operates them, how they are regulated and the quality of the medical care they provide…
County health officials describe the clinicas as a parallel health care system, servicing a vast number of uninsured Latino residents, yet the officials say they have little understanding of who owns and operates them, how they are regulated and the quality of the medical care they provide…
Visits to more than two dozen clinicas in South Los Angeles and the San Fernando Valley found Latino women in brightly colored nurses scrubs handing out cards and coupons that promise everything from pregnancy tests to tubal ligations. Others advertise evening and weekend hours, and, some 24-hour a day operations trumpet that they are “nunca cerramos” — never closed. That all-hours access — and up-front pricing — is critical, Latino health experts say, to a population that often works low-wage, around-the-clock jobs.
Also important, officials say, is that new immigrants from Mexico and Central America are more accustomed to a corner clinica, which is common in their home countries, than to the sprawling medical complexes or large community health centers found in the United States. And they can get the kind of medical treatments — including injections of hypertension drugs, vitamin solutions delivered intravenously and liberally dispensed antibiotics — that are frowned upon in traditional American medicine. (KHN/NYT)
Re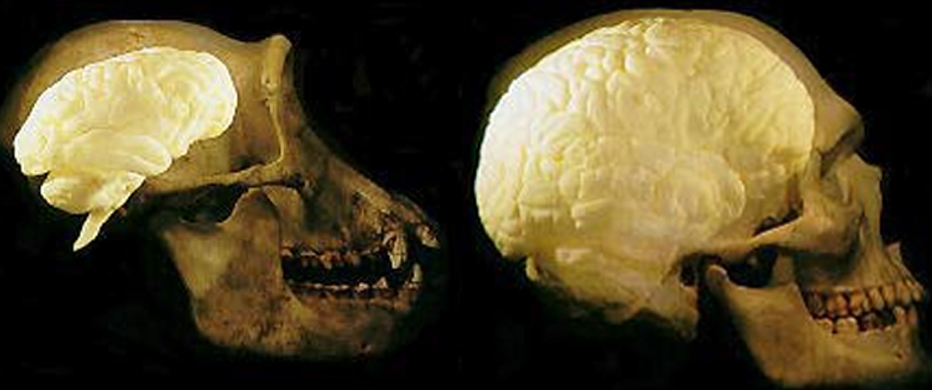 lative to body size, our brain is three times the size of a chimpanzee’s brain.
lative to body size, our brain is three times the size of a chimpanzee’s brain.
New study: Medicaid can account for at least eight percent of the decline in nonwhite child mortality from 1965 to 1979. HT: Tyler Cowen.
German hospitals promise pain free operations.
CMS: ObamaCare slowed health care spending last year, but it will increase spending this year.
Thousands of people are cramming in tests, elective procedures and specialist visits before year’s end, seeking out top research hospitals and physician groups that will be left out of some 2014 insurance plans under the new health law, health-care providers say.
Health insurers are especially focused on paring academic teaching and research hospitals from their networks because they generally charge more than community hospitals for similar services. [See chart]
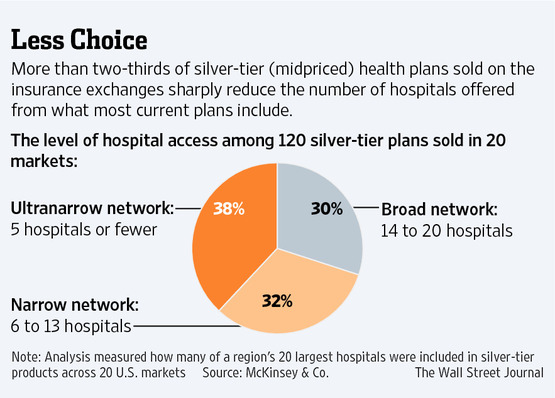
Source: WSJ.