Is Your Doctor a Happy Camper?
 Physician is arguable the profession with the highest average pay for all those pursuing it. Yes, some doctors lament that investment bankers often earn much more. But investment banker isn’t a profession; it’s a high-paid specialty in the area of banking. The average banker does not enjoy the income the average physician has come to expect.
Physician is arguable the profession with the highest average pay for all those pursuing it. Yes, some doctors lament that investment bankers often earn much more. But investment banker isn’t a profession; it’s a high-paid specialty in the area of banking. The average banker does not enjoy the income the average physician has come to expect.
Yet a new survey of physician incomes by Medscape finds only about half believe they are fairly compensated, with a slight majority of primary care physicians feeling like they’re getting the shaft. Dermatologists (64%) and Emergency Room physicians (61%) are the most likely to feel fairly compensated. Plastic surgeons (37%) and pulmonary physicians and neurologists (both 39%) feel the least fairly compensated.
Internists (71%) and family medicine physicians (73%) and pulmonary physicians (69%) are the most likely to report they would choose a career in medicine if they had it to do all over again. Plastic surgeons (47%), Orthopedists (49%) and Radiologists (49%) are among the least likely to report they would choose a medical career again. Interestingly, the physicians who report being happy about their decision to go into medicine are among the lowest paid physicians, while those who (supposedly) regret their decision are among the highest paid. However, the grass is always greener… Nearly three-quarters of the happy doctors working in internal medicine and family medicine would choose a different specialty if they could make the choice again. The unhappy docs working in plastic surgery and orthopedics are happy with their choice of specialty — if not their decision to pursue a medical career.


Also interesting: 26 percent reported exchanges had decreased their incomes, only 11 percent reported increase. It would have been better to separate the question about accepting Medicare and Medicaid patients into two questions, because other sources show Medicare acceptance is usual but Medicaid not. Also, it looks like concierge medicine or cash-paying practices continue to be a tiny share of practices.
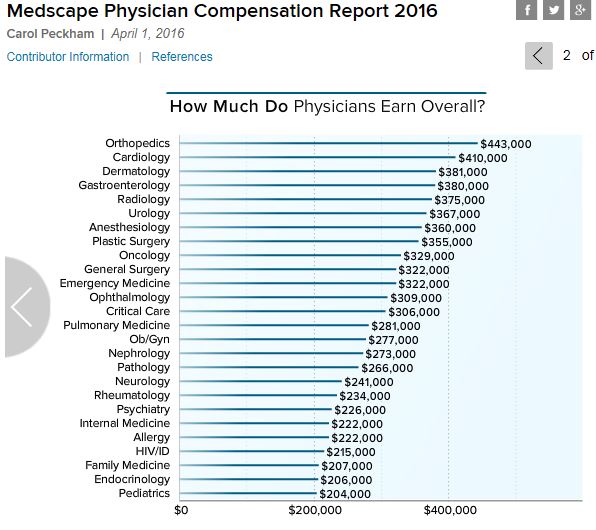
Is this average salaries? I suspect so, but would have preferred to see the median salaries as there is such a wide spread between high earners and low earners that it might make the salaries appear higher than they are for the general population.
I believe these are averages. The entire survey is worth looking at. I only touched on a tiny segment.
I agree – but I would still like to know how much variation there is within the reported averages. Medan incomes would be helpful – so would variance or standard deviation.
As far as I can tell, we’re still attracting plenty of well qualified applicants who want to attend medical school to become doctors as well as doctors from other countries who want to practice in the United States. I also note that there is a lot of psychic income associated with being a doctor and many view it as a calling and not just a job or a profession. Finally, compensation for a given specialty can vary quite significantly from one region to another. Metro areas where most doctors and their spouses prefer to live often have a disconnect between living costs and compensation but doctors, like many other people, are willing to make some financial sacrifices to live in an area that they find desirable as opposed to a less desirable area where they can make more money or afford a bigger house. If there are sub-specialties with chronic shortages of doctors due to inadequate compensation, I would be among the first to suggest that compensation needs to be increased.
Something else the survey showed was that doctors are talking to their patients about the cost of medical care.
o About 30% said they regularly discuss medical costs with patients
o Another 35% said they do under certain circumstances
o An additional 20% said they do if the patient brings it up.
That adds up to 85% who talk to patients about costs; and two-thirds who either do it regularly or when needed without the patient raising the topic.
Devon – That’s hopeful and welcome news toward helping to control healthcare costs over the intermediate to longer term.
On another front, I was at a meeting last weekend with a religious leader who was talking about issues affecting baby boomers including end of life care. He has done a lot of work and counseling on these issues over the last several decades and has a radio show in Philadelphia that addresses these topics.
After his talk, I asked him about whether or not more seniors are executing living wills and advance directives these days as compared to 10-15 years ago. He said the numbers are way up mainly because they’ve been through the end of life minefield with their own parents and they want their kids to have an easier time of it than they had.
Former Oklahoma Senator Coburn was an advocate of subsidizing end of life discussions between doctor and patient. I don’t recall the details, but as I believe his bill was willing to compensate Medicare beneficiaries for having the discussion and reimburse the doctor.
I believe another reason these discussions are taking place is because the good old days when nature would take its course have largely disappeared. Nobody wanted to make the decision to deny grandma care — preferring her to die a week or two later on her own. Now a week or two has turned into a month or two or a year or two.
“helping to control healthcare costs
No doubt that having a living will is a good thing. It is, however, something where the government should remain in the periphery. We should be looking at the living will as a personal decision and not one that can lead to savings.
It should be the family’s choice. The government should remain on the periphery and merely inform seniors Medicare will go after their estate for all charges for the last two weeks of care. Under those conditions I am willing to bet more families would make living wills and request hospice care.
* wink, wink
My doctor prefers glamping, but he’s an orthopedist, so apparently he can afford it.