Are Price Controls Disguised as Bundles the Next Step in Bending the Medical Cost Curve?
Fresh from reimaging health insurance, mainstream health policy analysts have now set their sights on the way that people who provide medical care are reimbursed. Initial indications are that this will not go well for patients. Academics and government agencies seem imbued with the conviction that every medical procedure in America costs twice as much as it should due to “flat of the curve medicine,” and that vast fortunes can be saved simply by chopping reimbursements.
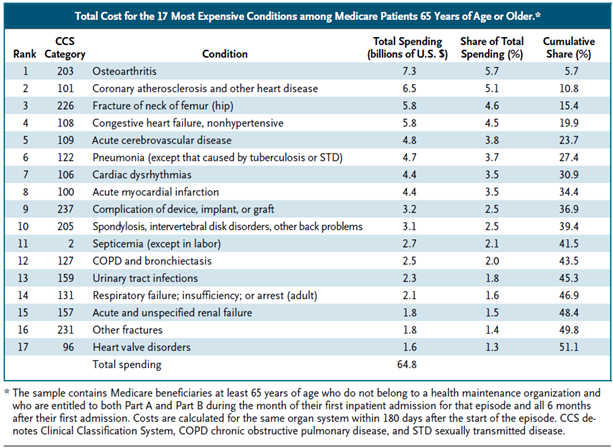
The table below lists Medicare’s 17 most expensive conditions. It is from a paper on reducing costs by changing Medicare payments from patient based payments to “bundled episode payments.” The authors argue that this reform could save $10 billion a year. They implicitly assume that higher average payments per patient “episode of care” in the 306 hospital referral regions that make up the upper 75th percentile of the payment distribution have no value. Given that, if one caps Medicare payments for each “episode of care” at the 25th percentile of the average cost per patient episode, one saves a great deal.
This is like saying that housing costs can be reduced by giving the federal government the power to decree that no one can spend any more on housing than the people living in Detroit.
Episode based payment is a compromise between paying a fee for services actually rendered and the capitated payments that pay a flat fee for all of the health care provided to each person every year. Compromise is needed because although mainstream health reformers irrationally dislike fee-for-service payments, they cannot deny that a flat fee structure harms the most seriously ill.
An episode would begin after the first hospitalization to treat an “organ system” provided there has been no hospitalization related to the same organ system within the previous 180 days. A single payment, based on recorded averages, would be made for all inpatient and outpatient spending occurring up to 180 days after the first hospitalization.
The problem with arbitrarily setting payments for knee replacements at the 25th percentile of the averages in specific geographic regions is that expenditures give no clue about whether there is room to reduce costs or whether the prices Medicare sets accurately reflect real costs. If a health problem is well understood, the medical system has a lot of experience curing it, there are a lot of physicians and facilities treating it, and the market is large enough to take advantage of supplier economies of scale, then existing suppliers may already be providing services using the fewest resources required to produce an acceptable outcome under current conditions. Arbitrarily seeking to lower expenditures by paying suppliers less without changing the knowledge base, the regulatory structure, or the cost of essential inputs like available labor would create shortages or degrade quality.
Neither the table nor health system reformers discriminate between cures that are efficiently provided, cures that are genuinely expensive due to the resources needed to provide them, cures that are costly because individuals vary so much that no one has yet managed to invent a standardized process that works, or cures that cost a lot because the regulatory constraints limit competition or regulators have picked an incorrect price.


Don’t forget the safety valve represented by the Mexican border.
If you find Obamacare pricing too expensive, you can get a fabulous deal by canceling Obamacare and heading for Mexico, Costa Rica, Brazil, Argentina, Hungary, Czech Republic, India and Thailand, all of which offer world-class care for between 1/9th and 1/2 the USSA prices.
In fact, you can get your dental care there, too, and it is recognized that two of the best countries for cosmetic surgery are Argentina and Brazil.
I just had cataract surgery done here in Rio de Janeiro for half what I was quoted in Austin, TX. What’s more, we have lots of limes that are free or almost so!
Medical Tourism is your friend.
A procedure in Ukraine would probably be pretty cheap right now
Hmm, or Juarez
Have y’all ever heard of Costa Rica, which doesn’t even have a military, and, unlike the USSA, hasn’t invaded a foreign country in decades? Son idiotos Ustedes.
Based on this, no one will want to take care of very sick patients.
No one does already! If they live alone and have no living family, who will pay off all their bills?
Uncle same of course!
It is an important realization to understand that there is no way to cut costs without changing the knowledge base. If we try to do as such, we will create disruptions in the market that will negatively affect the industry. Considering this premise, it is a bad omen for Obamacare. If we are dramatically increasing the number of consumers (demand) without increasing the amount of medical facilities (supply) we will create a shortage that is going to be large enough to cause a disruption in the market. And in a market as essential as the healthcare industry, a major rupture will have negative consequences to the economy as a whole.
Changing the knowledge base is one of the hardest and most expensive things to accomplish
I propose that we mandate that spending on forest-fire control in Oregon, Washington, Idaho, etc be normalized to the same levels as Nebraska, Kansas, and North Dakota on a per-acre basis.
That makes every bit as much sense as pretending that the vast demographic chasm that separates the health, wealth, education, and family/social-support networks for the average senior in, say, Utah and Louisiana have no effect on the amount of resources required to treat a given stroke patient during the initial hospitalization and especially during post-operative/home-care.
The bundles are never going to work
The GOP is looking for any way to seem smarter
I think the bundles are a lot like buying in bulk vs small amounts. Sure it’s cheaper to buy in bulk, but not everyone can afford the capital needed to do so.
Costco is a perfect example of that
I would like to believe that individual prices of surgeries would not go up, but that would be a key motivator to pick the packaged surgeries
Oh but they will